 (044) 3310767481
(044) 3310767481The Gastric Bypass (BPG) is a surgical procedure for the treatment of obesity categorized as MIXED, since it combines a restrictive element (decreases the amount of food that can be ingested), with a malabsorptive component (it does not allow most of the ingested food be absorbed by the body). It is the oldest operation, since 1966, it has passed the test of time, being the only operation that has been carried out for more than 30 years. It is considered the “Golden Standard” of obesity surgery and in recent years many details have been improved that make it safer and more effective.
Mechanism of Operation and Surgical Technique
Operations against obesity are categorized into two types: Restrictive and Malabsorption. The first category (restrictive) limits the amount of calories or food ingested, reducing the stomach space available to accommodate food. The second, malabsorption, reduces the absorption of food that has already been consumed. Gastric bypass surgery combines a gastric restriction procedure with a small portion of malabsorption.
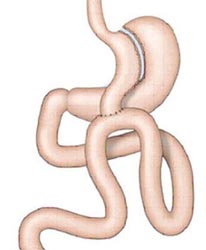
The surgeon reduces the size of the stomach, dividing it into a small upper bag that will act as a “new stomach” and a larger lower section, using a special stapler. After dividing the stomach, the surgeon connects the small intestine to the small pouch that will act as a “new stomach”, so that the flow of food skips the lower portion of the “former stomach”.
Benefits
–
–
–
-The person experiences a change in eating habits, due to the “gastric evacuation syndrome” (nausea, sweating, weakness and diarrhea) that will induce the consumption of foods with high caloric content. This syndrome is caused by any overdose of calories that reaches the small intestine.
- As the stomach becomes smaller, the person experiences a more rapid feeling of fullness.
- Also when a stomach is smaller, the person naturally reduces the amount of food they eat.
- The cancellation of an important part of the digestive tube produces mal-absorption of calories.
- The person experiences a change in eating habits, due to the “gastric evacuation syndrome” (nausea, sweating, weakness and diarrhea) that will induce the consumption of foods with high caloric content. This syndrome is caused by any overdose of calories that reaches the small intestine.
Achievements
- Patients lose two thirds of their excess weight in two years, 60% in 5 years, and more than 50% in 9 years.
- It is a very effective method to fight against morbid obesity, especially in patients addicted to sweets.
Gastric Bypass by Laparoscopy 
Laparoscopic surgery is a surgical technique that involves performing operations of organs inside the abdomen or the wall of the abdomen, through support with cameras, lighting and small-sized lenses that transmit the images to monitors, where The surgeon observes and through which he performs the desired surgery. Since 1988 it has been carried out around the world, it is a well-known technique that has progressively been improved, it has been applied to different pathologies and different organs, supported by the constant improvement of equipment and instruments, as well as in the design of new technology that makes it possible to perform more complex surgeries, with highly satisfactory results.
Advantage
- All of the gastric bypass have very good weight loss in most patients for many years.
- A low rate of long-term reoperations.
- All should be done laparoscopically (minimal scar, minimum pain, early discharge).
Disadvantages
- Higher cost in instruments.
- It can be very difficult or impossible in super obesity.
The maximum weight loss is achieved before 18 months with all interventions. On each intervention an author gives different figures on weight loss.
Not only weight is lost but co-morbidities are improved, such as diabetes, obesity-related apnea syndrome, hypertension and elevated cholesterol and triglyceride abnormalities. It also improves cardiac function and the size of the cardiac wall. Other important benefits are the improvement of mobility and resistance in general. Improves self-esteem, humor, interpersonal relationships, the ability to work and find work. The change that the individual has of his body image allows him to explore social, vocational and personal relationship activities. There is an important improvement in couples relationship, if they were good beforehand.
The effects on health and well-being in short and long term are extraordinary. Adult diabetes is cured, hypertension is improved or cured, sleep apnea disappears, many sterile patients become pregnant, urinary incontinence is corrected, joint pain is improved, etc.
MEDICAL AND NUTRITIONAL FOLLOW-UP
Gastric restrictive operations need education, motivation and cooperation of the patient to maintain an adequate intake of proteins, calories, minerals and vitamins. At 3 months there is a moderate protein deficit that disappears at 18 months, when the final weight has already been restored. Diets depend on the type of operation. Operations with rings force for life style change that restric the quality of meals and what they eat (meat, bread, dry rice, etc.). Mixed operations, as they do not use rings, have a better quality of life and diets. The gastric bypass is between the two extremes.
All restrictive operations, simple operations, force the patient to chew very well and very slowly if they do not want to vomit. In the first 3 months, if they vomit a lot, they may suffer mild overall nutritional deficits. In bypass and mixed operations, we must be careful that patients do not develop iron deficiency, anemia, Vitamin B12, calcium and fat-soluble vitamins. Therefore, it is desirable to carry out a continuous analytical follow-up so that if deficits are detected, they can be replaced. Malabsorption techniques have as a side effect the bad odor of feces.
FREQUENT QUESTIONS
- What is the recommended operation? How it is performed?
It should be discussed specifically with your surgeon. Pros and cons. Risks Ways to carry it out, etc.
- How does weight loss work?
In simple and restrictive stomach operations, reducing the amount of food that can be eaten, because the stomach is smaller and fills up more quickly. By eating less you lose weight.
- Does the intervention have risks?
All surgeries have risks. Bariatric surgery, which is a major surgery, is no exception. However, today it has less risk than most operations, and the risks of the operation is much lower than those of the untreated obesity disease. Each surgeon must explain the risks of each operation performed.
- How long will I be in the hospital?
Normally between three and five days, depending on how quickly you recover. The important thing will be long-term success.
- How long does it take to perform the operation?
It depends on each individual and the technique used. It can take anywhere from 45 minutes to 4 hours.
- Can I have the staples removed in the future?
The staples are permanent. The rings can be removed if necessary. All operations are reversible, but in principle all operations are for life because if the operation is undone the patient immediately regains weight.
- When can I go back to work?
Between 2 and 6 weeks. But you can not lift weights to avoid hernias.
- Will I have to follow a diet?
The diet after surgery is mandatory. In other words, you will not be able to eat certain foods, changing your eating habits by having to chew very well and eat slowly.
In mixed operations dietary restrictions are minimal.
- But … how much can I eat?
-Initially about 60 cc per meal. With time it increases to 150-200 cc. You must eat at least three times a day.
- With so little food, will I die of hunger?
You will be given a dietary program to cover your nutrition and vitamin needs.
- At what rate do you lose weight?
It depends on each person and the type of operation. It is not uncommon to lose 11 lb each month at the beginning for the first 12-18 months.
- What percentage of success does this surgery have?
It depends on the individual and the technique used. It is considered a success if half of the excess weight is lost. Most interventions surpass it. In some interventions some patients recover some of the weight lost. No intervention gives 100% success to patients.
- Why surgery?
Because the severe obese, who has tried all kinds of diets and failed, who has a “serious” disease, who has other serious medical problems (hypertension, diabetes, arthritis, heart disease, etc.) needs to lose weight and surgery is the most effective.
- Do I have to worry about my weight forever?
YES. Surgery gives a mechanical means to control what you eat and your weight, but you are not cured of your illness. Needing your full effort and adjustment to your lifestyle.
- Can a patient sabotage this surgery?
If you propose to, YES. In some operations more than in others. It is known of patients who take all the food in liquid creams and regain their weight. Surgery is only the beginning.
- What happens if I do not follow the program well?
At first if you insist on eating you will vomit. If you eat continuously you are going to make the stomach expand. If you continue the staples will come on done and you’ll gain weight again.
- I have heard that many patients vomit very often
Not necessarily if you follow the instructions. In ring operations if you try to eat solids without chewing first, it can bring you problems. In operations without a ring, patients tolerate better the intake and do not suffer from vomiting.
- How do I stop losing weight?
When you reach the balanced weight, which in advance can not be predicted, the organism is readjusted to the new intake and the weight is maintained. The weight loss is fat and not the noble parts of the body (muscles, vital organs such as liver, kidney, heart)
- Can you redo this operation again and again?
Obesity operations are permanent. All can be undone. Some patients need reoperations if they continually “break” the line of staples or make their stomach big again.
- I have heard that obesity operations are very dangerous
The operations of the intestinal short circuits were at long term, and today they are no longer done.
- Will I have skin flaps?
It is difficult to predict which patients will end up with flaps. It depends on the weight lost, on the elasticity of the skin and in women if they have had several children.